Crohn’s Disease and Ulcerative Colitis
 Crohn’s Disease and Ulcerative Colitis are both inflammatory bowel diseases (IBD) and as such respond well to hyperbaric oxygen therapy (HBOT) which has anti-inflammatory, bacteriostatic and pain reducing effect.
Crohn’s Disease and Ulcerative Colitis are both inflammatory bowel diseases (IBD) and as such respond well to hyperbaric oxygen therapy (HBOT) which has anti-inflammatory, bacteriostatic and pain reducing effect.
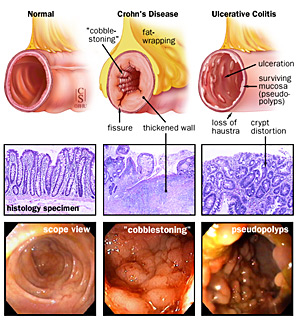
The infection and immune attack on normal mucosal bowel flora may affect any part of the gastrointestinal tract, but in Crohn’s the distal ileocecum, small intestine and colon are most commonly involved. Defects in intestinal epithelial cells lead to regional inflammation and ultimately in development of wounds, ulcers, deep fissures and enteric fistulae with risk of perforation within skin, bladder, vagina and other parts of bowel. In local infection hyperbaric oxygen therapy plays an important role in direct effect on bacteria elimination as well as boosting effects of antibiotics and immune system response. Hyperbaric oxygen therapy promotes oxygenation and blood flow to oxygen-deprived areas speeding the draining of the fistulas and wound closure with minimal scar formation. Oxygen promotes bone mineralization and has protective effect on the bones which are affected by long term steroid use.
Hyperbaric oxygen therapy is important in overall symptom improvement and reduced need for pain and anti-inflammatory medication in Crohn’s and Colitis.