Blood Loss and Anemia
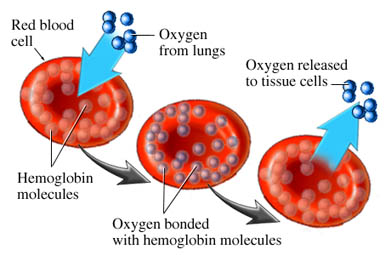
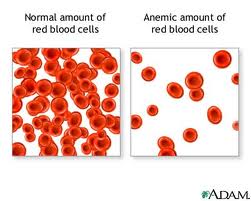
Acute blood loss, hemorrhage or anemia are characterized by significant decrease in blood volume and red blood cells – the main oxygen carriers in our body. Resulting lack of oxygen (hypoxia), if left untreated, can seriously harm the organ function. In acute or chronic anemia the body tries to compensate for decreased oxygen supply by producing more red blood cells in bone marrow and extract the liquid from interstitial places. Secondary carrier of oxygen in our body is blood plasma, with only 2% of carrying capacity when to compared to hemoglobin – protein in the red blood cell which carries oxygen.
The brain and heart are the most critical body tissues that require constant oxygen supply. In acute blood loss anemia the oxygen deprived tissues cause all blood vessels to open (dilate) to increase the blood flow. This will cause heart to work much harder and faster also to prevent cardiopulmonary congestion. Overworked heart in these conditions can lead to congestiveheart failure.
The treatment of severe anemia with hyperbaric oxygen is one of thirteen indications approved by the Hyperbaric Oxygen Therapy Committee of the Undersea and Hyperbaric Medical Society for appropriate use of the therapy. All publications report a positive result when hyperbaric oxygen is delivered as treatment for severe anemia. Oxygen therapy can be administered rapidly at pressure up to 2-3 ATA for periods of 3-4 hours three to four times a day if intra-treatment patient air breaks are used. In exceptional cases (Jehovah’s Witnesses and certain hemolytic anemias) when cross-matched transfusion is not possible, the intermittent use of hypetbaric oxygen dissolves enough oxygen in the severely anemic patient to support basic metabolic needs. Hyperbaric oxygen therapy at 3 ATA will place 6 volumes percent of oxygen dissolved in plasma for the direct use by tissue cells. At the same time the amount of stem cells released from bone marrow by 90 minute oxygen therapy doubles.
In chronic anemia such as in cancer patients oxygen treatments can be lengthened gradually until the hemoglobin baseline builds to allow for proper oxygen delivery. It has been shown clinically that a set of 20 sessions hyperbaric oxygen over 4 weeks will increase amount of stem cells in the blood circulation 8 fold. This is extremely important for those cancer patients who are awaiting bone marrow transplant. Harvesting of stem cells combined with hyperbaric oxygen therapy is becoming a routine in some medical centers.